This article looks at Tarong Nuclear and Accident impacts because a nuclear policy was released by the Liberal/National Coalition Party with a plant at Tarong coal power stations, co-located 26km southeast of Kingaroy.
- Accidents do happen. The best estimate is one every one or two decades.
- In a severe accident, the Sunshine Coast could be blanketed with a layer of contamination due to summer fast-moving thunderstorms wind patterns from the Toowoomba area for at least 5 months of the year..
- Contamination with Cs143 and St90 is for generations with a half life of 30 years..
- Wind can take contamination up to 1,000 km
- Low levels of contamination increases risk of childhood thyroid cancer even at moderate doses (~0.05 Gy) over 30 years
- Fukushima had lower cancer rates with hundreds of thyroid cancer cases. We are only at the 14-year mark with 30 years to go.
- The response to both nuclear accidents was inadequate, ill-prepared and were symptomatic cascading failures.
- People and lives are affected for generations.
Locations And Zones
Distance from Tarong to the boundary of Fairfax is 60km, Mapleton 92km and Maroochydore 117km.
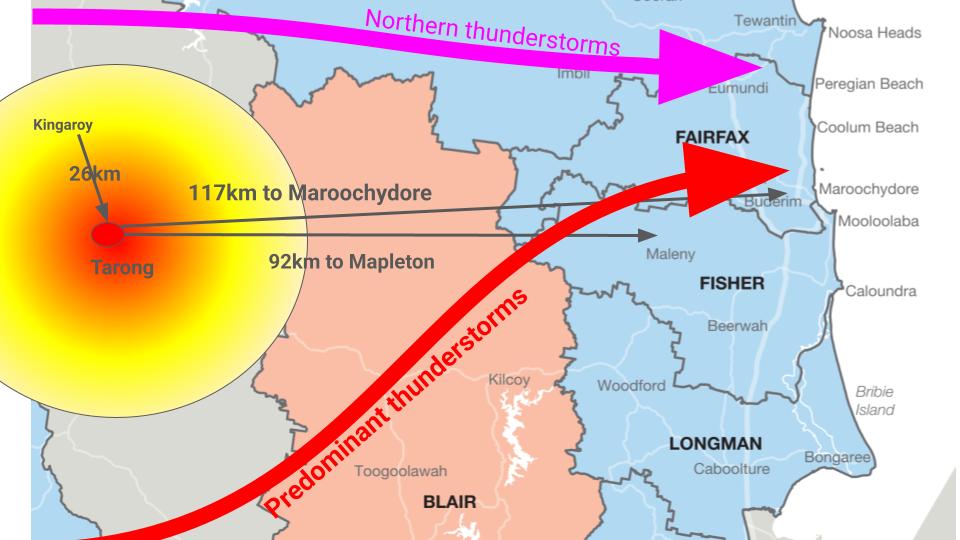
Figure 1 Location and predominant thunderstorm tracks for the Sunshine Coast
An evacuation zone of 30km radius was deemed appropriate for Fukushima and Chernobyl nuclear plant accidents. That zone is shown in Figure 1. As it turned out over the following 2 decades, these exclusion zones may have prevented immediate death. They did not stop the decades of cancers and illnesses, nor the economic losses.
Part of the higher rate of thyroid cancers in Chernobyl versus Fukushima was due to feeding milk to young people on milk from cows who had been eating contaminated pastures. In Fukushima, there was an immediate stop to agriculture in the exclusion zone.
Safety by Rhetoric
Nuclear is intrinsically unsafe. Safety between past reality and future claims is a mismatch by nuclear advocates. The trap of absolute safety of nuclear power is a myth [1] with Fukushima an example. Compare aeroplanes and nuclear reactors. Both planes and nuclear reactors need to do work to be safe. Planes are heavy objects that defy gravity to fly. Nuclear plants must contain the fission process under challenging conditions. High temperatures, high pressure, damage to materials from radiation create unsafe conditions. Neither of these is easily achieved under all circumstances. Planes crash. Reactors go out of control. [2]
The risk of an accident is one in a million years of operation.
I have lived through 3 major accidents.
The point is simple.
Theoretical predictions of stupefying low accident probabilities do not square with the empirical evidence of severe accidents at nuclear reactors. The statistics are beyond the scope of this [3] discussion.
Calculating Risks
Over the years there have been more than 99 “incidences” in nuclear plants. [4] Nuclear advocates say the risk is “close” to zero. Other researchers such as Lelieveld [5] say the true risk is an accident every one to two decades. Safety cannot be 100%. Accidents happen.
Lelieveld determined the likelihood of a nuclear meltdown by a simple calculation. They divided the operating hours of all civilian nuclear reactors in the world, from the commissioning of the first up to the present, by the number of reactor meltdowns that have actually occurred. The total number of operating hours is 14,500 years, the number of reactor meltdowns comes to four. One at Chernobyl and three at Fukushima. One major accident, being defined according to the International Nuclear Event Scale (INES), every 3,625 years. INES is a log scale, similar to that of earthquakes. That risk assessment is 200 times higher than the estimate for catastrophic, non-contained core meltdowns made by the U.S. Nuclear Regulatory Commission in 1990. [6].
With no serious meltdown since 2011, the number of operating hours has risen. Are accidents every decade or every two or three? What is clear that 14,000 thyroid cancer and 25,000 cancer sufferers don’t buy the myth of absolute safety. And neither should you and I.
Cascading Failure
A cascading failure is a failure in a system of interconnected parts in which the failure of one or few parts leads to the failure of other parts, growing progressively as a result of positive feedback. [6] An independent investigation panel of Fukushima showed [1]
- Safety layers were thoroughly unprepared on almost every level for the cascading nuclear disaster.
- Caused by the public myth of absolute safety
- Dysfunction within and between government agencies and Tepco
- The tsunami was not anticipated
- Ambiguity about the roles of public and private institutions in the crisis exacerbated a poor response and led to an estimated $211 billion economic hit.
Displacement by the authorities meant a sharp increase in deaths among elderly people who were put in temporary housing, as well as an increased risk of chronic diseases such as diabetes. Lack of access to health care in the temporary location likely was a key contributor to these effects. [7]
Exclusion Zones
There are 2 zones of note. One 15km area is where people could be harmed by direct radiation exposure. The second zone covers a broader 80 km radius – where radioactive materials could contaminate water supplies, food crops and livestock. Under US REGULATORY GUIDE 4.7 the exclusion area is required to be of such a size that an individual assumed to be located at any point on its outer boundary would not receive a radiation dose in excess of 25 rem total effective dose equivalent (TEDE) over any 2-hour period following a postulated fission product release.
The required exclusion area size involves consideration of the atmospheric characteristics of the site as well as plant design.
Post major accidents in Chernobyl and Fukushima, both EEC Japan and most states of the US there an additional 100 to 200km zones of agricultural control around their nuclear stations such that if there is steam or gas escape then movement of agricultural products must cease immediately until it is shown that there is no radioactive plume.
Analysis from both Fukushima and Chernobyl revealed that, on average, only 8% of the CS137 particles deposited within an area of 50 kilometres around the nuclear accident site. Around 50% of the particles were deposited outside a radius of 1,000 kilometres, and around 25% spread even further than 2,000 kilometres. These results underscore that reactor accidents are likely to cause radioactive contamination well beyond national borders. At Fukushima, 90% of the particles were blown out to the Pacific Ocean. Low levels of radiation were detected in Oregon, USA. Had the wind been more normal, Tokyo would have needed to be evacuated.
Prevailing Winds and Thunderstorms
The prevailing wind on the Sunshine Coast is a cool south-easterly wind that blows for 8 months of the year and to the largest extent why the Sunshine Coast has a very favourable climate, given its latitude. The SE wind keeps the Coast cool, and Gympie which does not get the same wind is 3 degrees warmer. That reduces the risk of contamination from Tarong.
South-East Queensland is a region that is particularly susceptible to severe thunderstorms, especially during the summer months. For example, the highest recorded wind gust from 48 years of data at Brisbane airport occurred during a severe ‘supercell’ thunderstorm in January 1985. [8]. Thunderstorms can move fast at over 40kph and a thunderstorm monitored in Toowoomba can be on the coast in under 1 hour. The typical Sunshine Coast thunderstorm develops in the Granite belt south of Toowoomba and moves north east. Depending on the storm, it crosses the coast from Brisbane to Coolum. The path of this is shown in Figure 2.
For 20% of the Sunshine Coast storms, the storm builds in the Kingaroy area and moves south east and dumps on Noosa south to Coolum, occasionally as far south as Caloundra.
Callaghan studied 48 events spanning 29 years of SE Qld thunderstorms. [9]. In this image here, the Sunshine Coast gets some of these stormsSupercells may have a lifespan of several hours and present an impact front as wide as 40 km.
Map of SE Queensland Storms
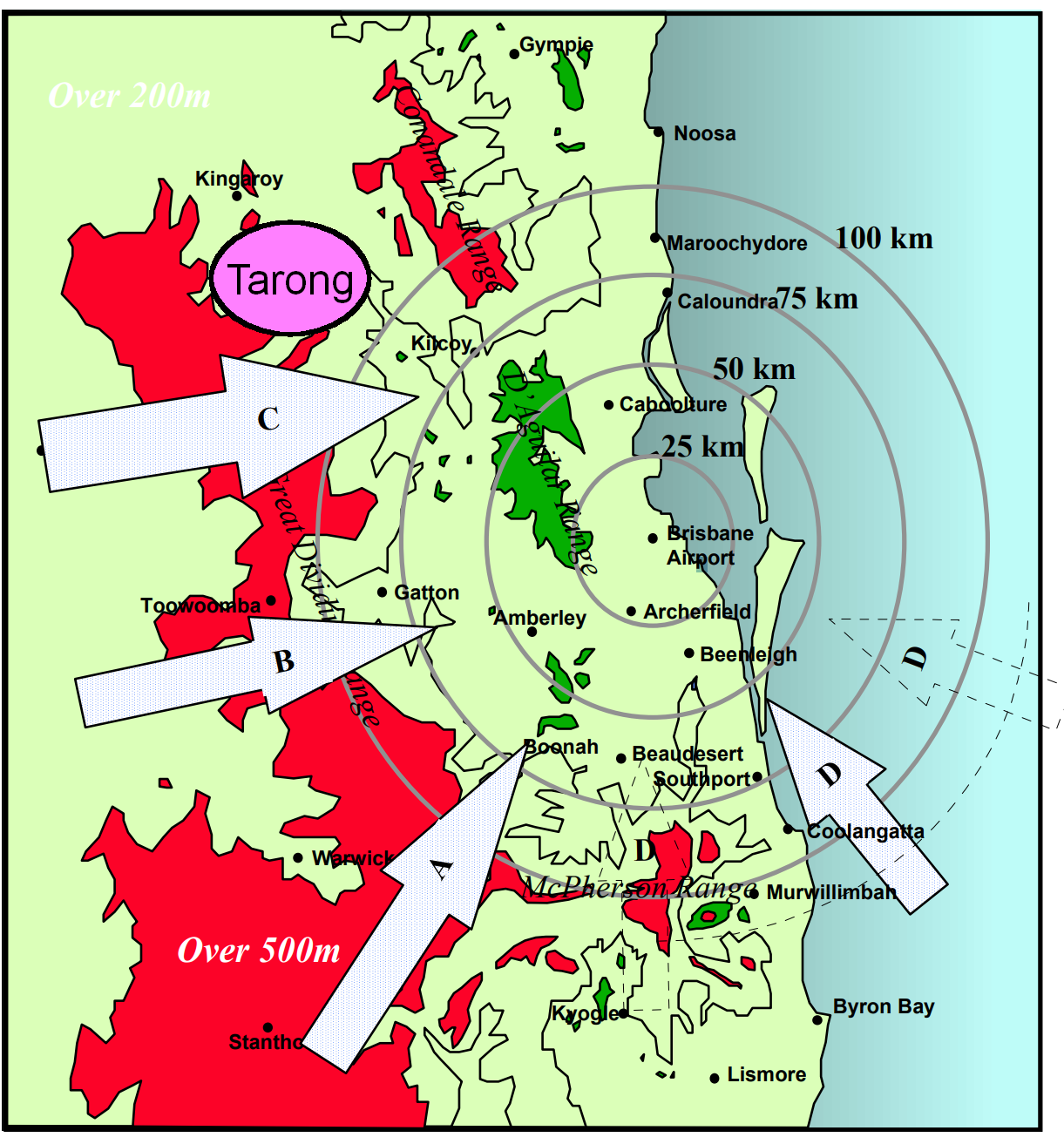
.Figure 2: synoptic track classes from Harper and Callaghan 1998
Callaghan also proposed a strong association between both storm intensity and track as a function of the regional topography; these being related to:
- The highland regions to the south and west provide elevated convective heat sources and hence buoyant air;
- For storms to reach the coast, a generally westerly steering current at middle levels and providing vertical wind shear is needed to sustain severe storms;
- Low-level convergence on the coastal plain, which compensates for the loss of buoyancy in moving off the ranges;
- The interaction between the sea breeze and frontal/trough systems generates and intensifies severe thunderstorms in the populated coastal plains region.
More recent work for the Brisbane region [9] shows the predominant wind is SWEST (1956-1997). Tarong is further north than the typical path, but storms also come from the Kingaroy region, passing the Tarong area and coming down over the Sunshine Coast, often with Noosa and Coolum in its path.
There is a 130% increased risk of thunderstorms in non-El Nino years [10]. It is clear that future years with climate change will bring more frequent and stronger El Nino events [11]. Climate change will be associated with stronger and more frequent storms.
1. Thyroid Cancer Risks
Chernobyl Cancer Evidence
- Chernobyl Evidence:
- About 31 people died at Chernobyl, and 600,000 liquidators were exposed. The government evacuated 115,000 people from the most heavily contaminated areas in 1986, and another 220,000 people in subsequent years.
- Strong evidence links iodine-131 exposure in children (<18 years old) to a linear increase in thyroid cancer risk, with a dose-response relationship of excess relative risk (ERR) per Gy of 1.91 [12], [13], [14]
- The International Agency for Cancer, WHO, say by 2065, models predict that about 16,000 cases of thyroid cancer and 25,000 cases of other cancers may be expected due to radiation from the accident with over 16,000 deaths [15]
- Risks persisted for decades without attenuation over time and were observed even at low doses (e.g., ~0.05 Gy I-131 thyroid dose) [12], [13] .
- Exposure to contaminated food and inadequate iodine prophylaxis were critical factors in amplifying risks [13], [14], [16]
Fukushima Thyroid Observations
- Fukushima Observations:
- Thyroid doses among the majority of Fukushima residents were low (most ≤10 mSv; maximum ~30-50 mSv) due to effective countermeasures (evacuation, food controls) [17], [18], [19], [20]
- Large-scale systematic screenings through the Fukushima Health Management Survey (FHMS) detected high thyroid cancer prevalence, but the excess is attributed to overdiagnosis and screening effects, with no direct evidence of radiation-induced thyroid cancers [17], [21], [22]. This conclusion is at odds with the observations. There was a 30 fold increase in thyroid cancer cases in children and adolescents with over 266 surgeries to remove their thyroid. These patients require lifelong ingestion of thyroid with a poorer quality of life, such as insomnia and fatigue.
- The close relationship between TEPCO (Tokyo Electric Power Company) and the Government directly caused the severity of the accident. During construction engineers recommended the sea wall to be 2 m taller – the Government waived that engineering recommendation.
- The attribution of “overdiagnosis” by TEPCO and UNSCEAR is at odds with best practice that with most cancers, early detection of cancers reduces fatalities. [23] [24] “Overdiagnosis” will have improved early detection, and avoided fatalities.
2. Broader Cancer and Health Outcomes:
- Cancer takes a long time. Short-term conclusions (less than 20 years) are meaningless. The half life of 30 years for CS134 and St90 suggests conclusions need to be made after 30 or 45 years.
- Non-Thyroid Cancers: Evidence for increased risks of cancers other than thyroid cancer from low-dose exposures (≤100 mSv) in Chernobyl and Fukushima populations is limited or inconclusive [17], [21], [25] say these reports, yet the WHO Cancer report explicitly states some 25,000 future cases are predicted.
- Mental and Physical Health: Psychosocial stress, lifestyle changes (e.g., metabolic disorders), and psychological distress were prominent in Fukushima but unrelated to radiation exposure itself [18], [21], [22], [26]
3. Impact on Broader Environment
A review of over 521 papers following Chernobyl showed elevated radiation levels recorded among a diversity of species, even up to thousands of kilometres away from the meltdown site, and after more than two decades following the accident. [27]Close to the reactor, physiological and morphological changes occurred with negative effects on the ecosystem, including contamination of water, soils, and wild food supplies.
4. Radiation Dose Contexts
In presenting radiation and dose measures, we have to understand the units of measure. Any discussion should be about the SI units (but you will see other measures, especially from the USA).
| SI Units* | Common Units | |
| Radioactivity | becquerel (Bq) | curie (Ci) |
| Absorbed Dose | gray (Gy) | rad |
| Dose Equivalent | sievert (Sv) | rem |
| Exposure | coulomb/kilogram (C/kg) | roentgen (R) |
The Cs137 isotope is a product of the nuclear fission of uranium. It has a half-life of 30 years and was one of the key elements in the radioactive contamination following the disasters of Chernobyl and Fukushima. Note that there were over 100 radioactive elements. Most are short-lived and decayed (reduced in radioactivity) very quickly. Iodine, strontium and caesium were the most dangerous of the elements released and have half-lives of 8 days, 29 years, and 30 years respectively. St90 and Cs137 are, therefore, still present in the area to this day.[28]
Radioactivity On Sunshine Coast
In a European study, the computer simulations revealed that, on average, only 8% of Cs137 particles are expected to deposit within an area of 50 kilometres around the nuclear accident site. Around 50% of particles would be deposited outside a radius of 1,000 kilometres, and around 25% would spread even further than 2,000 kilometres. These results underscore that reactor accidents are likely to cause radioactive contamination well beyond national borders in Western Europe
In Western Europe, where the density of reactors is particularly high, contamination by more than 40 kBqm-3 is expected to occur once in about every 50 years.
The Tarong site would have multiple reactors. It is less than 100km to the Sunshine Coast. Summer storms and strong winds from Tarong to the Coast would carry radiation in less than 1 hour. Therefore, the Coast could reasonably expect similar levels of risk.
How Much is Too Much Radiation
- A single chest x-ray exposes the patient to about 0.1 mSv. This is about the same amount of radiation people are exposed to naturally over the course of about 10 days.
- A mammogram exposes a woman to 0.4 mSv, or about the amount a person would expect to get from natural background exposure over 7 weeks.
- A seven hour airplane trip exposes passengers to 0.02 mSv
Exposure at Nuclear Accident Sites
The amount of radioactivity released at these two accident sites is known. Note a PBq is a peta becquerel or 1 x 1015 or 1 followed by 15 zeros. It is a lot! When we look at what sort of dosage people have around Chernobyl or Fukushima, we can see that these events are orders of magnitude higher.
Chernobyl released 10 times more than Fukushima. But Fukushima, due to better monitoring by the Japanese authorities as opposed to the Ukrainian, knows 20% came from unit 1, 40% from unit 2 (peak on 15 March), and 40% from unit 3 (peak on 16 March). Releases to the ocean over 26 March to 30 September were about 11 PBq iodine-13, 3.5 PBq Cs-134, 3.6 PBq Cs-137, total 18.1 PBq (or 169 PBq I-131 eq) apart from atmospheric fallout. More than 90% went over the ocean, not across the land due to winds.
- Dose Differences Between Chernobyl and Fukushima:
- Chernobyl: Higher individual thyroid doses (often >100 mSv) (1,000 chest x-rays) due to delayed iodine prophylaxis and widespread contamination [12], [13], [14]
- Fukushima: Lower thyroid doses (<30 mSv) (300 chest x-rays) primarily reflected early evacuation and containment measures [17], [20], [21]
- Uncertainties: Fukushima dose reconstructions highlighted variability in early ingestion pathways for internal iodine-131 exposure, indicating areas for improved dosimetry models [19], [20], [29]
5. Policy and Research Implications:
- Screening Effects: Overdiagnosis from proactive monitoring (e.g., thyroid ultrasound) underscores the need to separate screening-detected cases from true radiation-induced cancers [17], [22]
- Low Dose-Response Debates: Risks at very low doses (<10-20 mSv) remain difficult to quantify, leading to ongoing debates over the applicability of linear dose-response models (e.g., LNT) [17], [30], [31]
6. Spread from the Chernobyl Disaster
What surprises most is the spread from Chernobyl. This figure 3 from 521 studies on ecological studies highlights the level of radiation. Note the size of the circle is the level of radiation at that particular site, some 20 years after Chernobyl.
Over 25 percent of the radioactive particles are transported further than 2,000 kilometres.
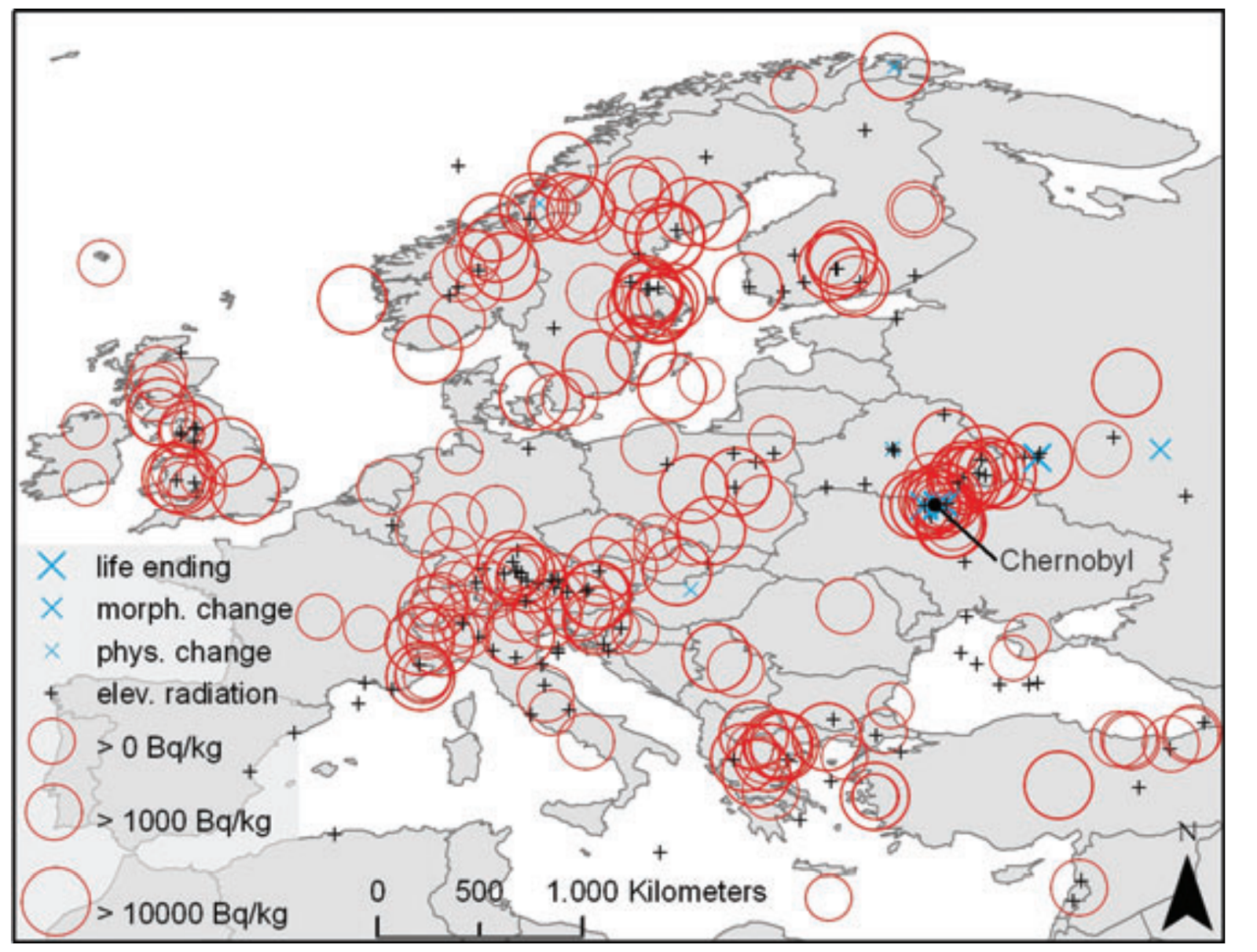
Figure 3 Spatial distribution of the impacts of the Chernobyl disaster described by the 521 studies included in the review (15 studies outside the western Palearctic are not shown). Bq/kg is the most common unit for the level of radiation. Thresholds for food items vary across countries but 600 Bq/kg is a common value set by many countries.
Conclusion:
- Accidents do happen. The risk is for every one or two decades, some 200 times more than the nuclear advocates promote incorrectly.
- The probability that the Sunshine Coast will be blanketed with a layer of contamination is high because fast-moving summer thunderstorms will take any accidental release at least over the whole of the Sunshine Coast. That an accidental release will happen when winds are blowing from the South East is an indication of criticality .
- The evidence and robust epidemiological evidence (e.g., from Chernobyl) confirms an increased risk of childhood thyroid cancer due to iodine-131 exposure, even at moderate doses (~0.05 Gy).
- Exposure health effects were not reported as significant for Fukushima residents, where exposures were much lower (~≤30 mSv). Given there were 30 times higher incidences and hundreds of thyroid cancer cases that seems bizarre. While authorities blame overdiagnosis rather than radiation-induced effects, those who had thyroid cancer were not just imagining cancer.
- People and lives are affected for generations.
References
[1] ‘Fukushima in review: A complex disaster, a disastrous response – Yoichi Funabashi, Kay Kitazawa, 2012’. Accessed: Feb. 20, 2025. [Online]. Available: https://journals.sagepub.com/doi/full/10.1177/0096340212440359
[2] ‘Nuclear is Not the Solution: The Folly of Atomic Power in the Age of Climate Change | Verso Books’. Accessed: Feb. 19, 2025. [Online]. Available: https://www.versobooks.com/en-gb/products/3013-nuclear-is-not-the-solution?srsltid=AfmBOoq-zOxZXp4fE96pFEZiyMy5Ua7WhbGHKZN5YphpS8zPOBcyPzug
[3] G. Keith, ‘The Two Schools of Probability Theory’, Medium. Accessed: Feb. 20, 2025. [Online]. Available: https://www.cantorsparadise.com/the-two-schools-of-probability-theory-76d0c0c8198d
[4] ‘Nuclear and radiation accidents and incidents – Wikipedia’. Accessed: Feb. 19, 2025. [Online]. Available: https://en.wikipedia.org/wiki/Nuclear_and_radiation_accidents_and_incidents
[5] ‘Severe nuclear reactor accidents likely every 10 to 20 years, European study suggests’, ScienceDaily. Accessed: Feb. 19, 2025. [Online]. Available: https://www.sciencedaily.com/releases/2012/05/120522134942.htm
[6] ‘Cascading failure’, Wikipedia. Mar. 23, 2024. Accessed: Feb. 20, 2025. [Online]. Available: https://en.wikipedia.org/w/index.php?title=Cascading_failure&oldid=1215159665
[7] ‘Fukushima Radiation Emergency: Lessons Learned | Radiation Emergencies | CDC’. Accessed: Feb. 20, 2025. [Online]. Available: https://www.cdc.gov/radiation-emergencies/features/fukushima.html
[8] B. Harper, K. Granger, and S. Hall, ‘CHAPTER 6: SEVERE THUNDERSTORM RISKS’.
And more Reading
[9] ‘(PDF) High-Impact Thunderstorms of the Brisbane Metropolitan Area’. Accessed: Feb. 19, 2025. [Online]. Available: https://www.researchgate.net/publication/340224177_High-Impact_Thunderstorms_of_the_Brisbane_Metropolitan_Area
[10] ‘Severe thunderstorms in the Brisbane region and a relationship to the El Niño Southern Oscillation’, ResearchGate, Oct. 2024, Accessed: Feb. 19, 2025. [Online]. Available: https://www.researchgate.net/publication/290317704_Severe_thunderstorms_in_the_Brisbane_region_and_a_relationship_to_the_El_Nino_Southern_Oscillation
[11] ‘Climate Change Now a Major Factor in Formation of El Niño – Yale E360’. Accessed: Feb. 19, 2025. [Online]. Available: https://e360.yale.edu/digest/el-nino-climate-change
[12] A. Brenner et al., ‘I-131 Dose Response for Incident Thyroid Cancers in Ukraine Related to the Chornobyl Accident’, Environmental Health Perspectives, vol. 119. pp. 933–939, 2011. doi: 10.1289/ehp.1002674.
[13] P. Jacob et al., ‘Childhood exposure due to the Chernobyl accident and thyroid cancer risk in contaminated areas of Belarus and Russia’, British Journal of Cancer, vol. 80. pp. 1461–1469, 1999. doi: 10.1038/sj.bjc.6690545.
[14] E. Cardis et al., ‘Risk of thyroid cancer after exposure to 131I in childhood.’, Journal of the National Cancer Institute, vol. 97 10. pp. 724–32, 2005. doi: 10.1093/JNCI/DJI129.
[15] ‘The Cancer Burden from Chernobyl in Europe WHO’. Accessed: Feb. 20, 2025. [Online]. Available: https://www.iarc.who.int/wp-content/uploads/2018/07/IARCBriefingChernobyl.pdf
[16] Y. Demidchik, V. Saenko, and S. Yamashita, ‘Childhood thyroid cancer in Belarus, Russia, and Ukraine after Chernobyl and at present.’, Arquivos brasileiros de endocrinologia e metabologia, vol. 51 5. pp. 748–62, 2007. doi: 10.1590/S0004-27302007000500012.
[17] S. Yamashita, S. Suzuki, S. Suzuki, H. Shimura, and V. Saenko, ‘Lessons from Fukushima: Latest Findings of Thyroid Cancer After the Fukushima Nuclear Power Plant Accident’, Thyroid, vol. 28. pp. 11–22, 2018. doi: 10.1089/thy.2017.0283.
[18] A. Kumagai and K. Tanigawa, ‘CURRENT STATUS OF THE FUKUSHIMA HEALTH MANAGEMENT SURVEY’, Radiation Protection Dosimetry, vol. 182. pp. 31–39, 2018. doi: 10.1093/rpd/ncy138.
[19] E. Kim, O. Kurihara, N. Kunishima, T. Momose, T. Ishikawa, and M. Akashi, ‘Internal thyroid doses to Fukushima residents—estimation and issues remaining’, Journal of Radiation Research, vol. 57. pp. i118–i126, 2016. doi: 10.1093/jrr/rrw061.
[20] S. Nagataki, N. Takamura, K. Kamiya, and M. Akashi, ‘Measurements of Individual Radiation Doses in Residents Living Around the Fukushima Nuclear Power Plant’, vol. 180. pp. 439–447, 2013. doi: 10.1667/RR13351.1.
Even More
[21] S. Yasumura et al., ‘Achievements and Current Status of the Fukushima Health Management Survey’, Journal of Epidemiology, vol. 32. pp. S3–S10, 2022. doi: 10.2188/jea.JE20210390.
[22] K. Kamiya, ‘Health management and care following the Fukushima nuclear power plant accident: overview of Fukushima Health Management Survey’, Annals of the ICRP, vol. 50. pp. 82–89, 2021. doi: 10.1177/01466453211015402.
[23] ‘The American Cancer Society challenge goal to reduce US cancer mortality by 50% between 1990 and 2015: Results and reflections – Byers – 2016 – CA: A Cancer Journal for Clinicians – Wiley Online Library’. Accessed: Feb. 20, 2025. [Online]. Available: https://acsjournals.onlinelibrary.wiley.com/doi/full/10.3322/caac.21348
[24] Thyroid Cancer Survival Rates. Accessed: Feb. 20, 2025. [Online]. Available: https://www.cancer.org/cancer/types/thyroid-cancer/detection-diagnosis-staging/survival-rates.html
[25] Y. F. Ali, F. Cucinotta, N.-A. Liu, and G. Zhou, ‘Cancer Risk of Low Dose Ionizing Radiation’, vol. 8. 2020. doi: 10.3389/fphy.2020.00234.
[26] K. Tanigawa, ‘Medical and health surveillance in postaccident recovery: experience after Fukushima’, Annals of the ICRP, vol. 47. pp. 229–240, 2018. doi: 10.1177/0146645318756819.
[27] H. von Wehrden et al., ‘Consequences of nuclear accidents for biodiversity and ecosystem services’, Accessed: Feb. 19, 2025. [Online]. Available: https://conbio.onlinelibrary.wiley.com/doi/10.1111/j.1755-263X.2011.00217.x
[28] ‘Frequently Asked Chernobyl Questions’. Accessed: Feb. 20, 2025. [Online]. Available: https://www.iaea.org/newscenter/focus/chernobyl/faqs
[29] Kimiaki and Saito, ‘Features of Exposure Doses to the Public due to the Fukushima Accident’. 2017.
[30] S. Nagataki and N. Takamura, ‘A review of the Fukushima nuclear reactor accident: radiation effects on the thyroid and strategies for prevention’, Current Opinion in Endocrinology & Diabetes and Obesity, vol. 21. pp. 384–393, 2014. doi: 10.1097/MED.0000000000000098.
[31] Y. Oghiso, ‘Health Risks of Low Dose-Rate and Low Dose Radiation Exposures’, Journal of Veterinary Epidemiology, vol. 16. pp. 1–3, 2012. doi: 10.2743/JVE.16.1.